Beat Easy to Cheat on Care Plan
Writing thebestnursing care plan requires a step-by-step approach to complete the parts needed for a care plan correctly. This tutorial has the ultimate database and list of nursing care plans (NCP) and NANDA nursing diagnosis samples for our student nurses and professional nurses to use — all for free! A care plan's components, examples, objectives, and purposes are included with a detailed guide on writing an excellent nursing care plan or a template for your unit.
What is a nursing care plan?
Anursing care plan (NCP) is a formal process that correctly identifies existing needs and recognizes potential needs or risks. Care plans provide communication among nurses, their patients, and other healthcare providers to achieve health care outcomes. Without the nursing care planning process, the quality and consistency of patient care would be lost.
Nursing care planning begins when the client is admitted to the agency and is continuously updated throughout in response to the client's changes in condition and evaluation of goal achievement. Planning and delivering individualized or patient-centered care is the basis for excellence in nursing practice.
Types of Nursing Care Plans
Care plans can be informal or formal: An informal nursing care plan is a strategy of action that exists in the nurse's mind. Aformal nursing care plan is a written or computerized guide that organizes the client's care information. Formal care plans are further subdivided into standardized care plans and individualized care plans:Standardized care plans specify the nursing care for groups of clients with everyday needs.Individualized care plans are tailored to meet the unique needs of a specific client or needs that are not addressed by the standardized care plan.
Objectives
The following are the goals and objectives of writing a nursing care plan:
- Promote evidence-based nursing care and render pleasant and familiar conditions in hospitals or health centers.
- Support holistic care which involves the whole person, including physical, psychological, social, and spiritual, with the management and prevention of the disease.
- Establish programs such as care pathways and care bundles. Care pathways involve a team effort to reach a consensus regarding standards of care and expected outcomes. In contrast, care bundles are related to best practices concerning care given for a specific disease.
- Identify and distinguish goals and expected outcomes.
- Review communication and documentation of the care plan.
- Measure nursing care.
Purposes of a Nursing Care Plan
The following are the purposes and importance of writing a nursing care plan:
- Defines nurse's role. It helps to identify the unique role of nurses in attending to clients' overall health and well-being without having to rely entirely on a physician's orders or interventions.
- Provides direction for individualized care of the client. It allows the nurse to think critically about each client and develop interventions directly tailored to the individual.
- Continuity of care. Nurses from different shifts or departments can use the data to render the same quality and type of interventions to care for clients, therefore allowing clients to receive the most benefit from treatment.
- Documentation. It should accurately outline which observations to make, what nursing actions to carry out, and what instructions the client or family members require. If nursing care is not documented correctly in the care plan, there is no evidence the care was provided.
- Serves as a guide for assigning a specific staff to a specific client. There are instances when a client's care needs to be assigned to staff with particular and precise skills.
- Serves as a guide for reimbursement. The insurance companies use the medical record to determine what they will pay concerning the hospital care received by the client.
- Defines client's goals. It benefits nurses and clients by involving them in their treatment and care.
Components
A nursing care plan (NCP) usually includes nursing diagnoses, client problems, expected outcomes, and nursing interventions and rationales. These components are elaborated below:
- Client health assessment, medical results, and diagnostic reports are the first steps to be able to design a care plan. In particular, client assessment is related to the following areas and abilities: physical, emotional, sexual, psychosocial, cultural, spiritual/transpersonal, cognitive, functional, age-related, economic, and environmental. Information in this area can be subjective and objective.
- Expected client outcomes are outlined. These may be long and short-term.
- Nursing interventions are documented in the care plan.
- Rationale for interventions to be evidence-based care.
- Evaluation. This documents the outcome of nursing interventions.
Care Plan Formats
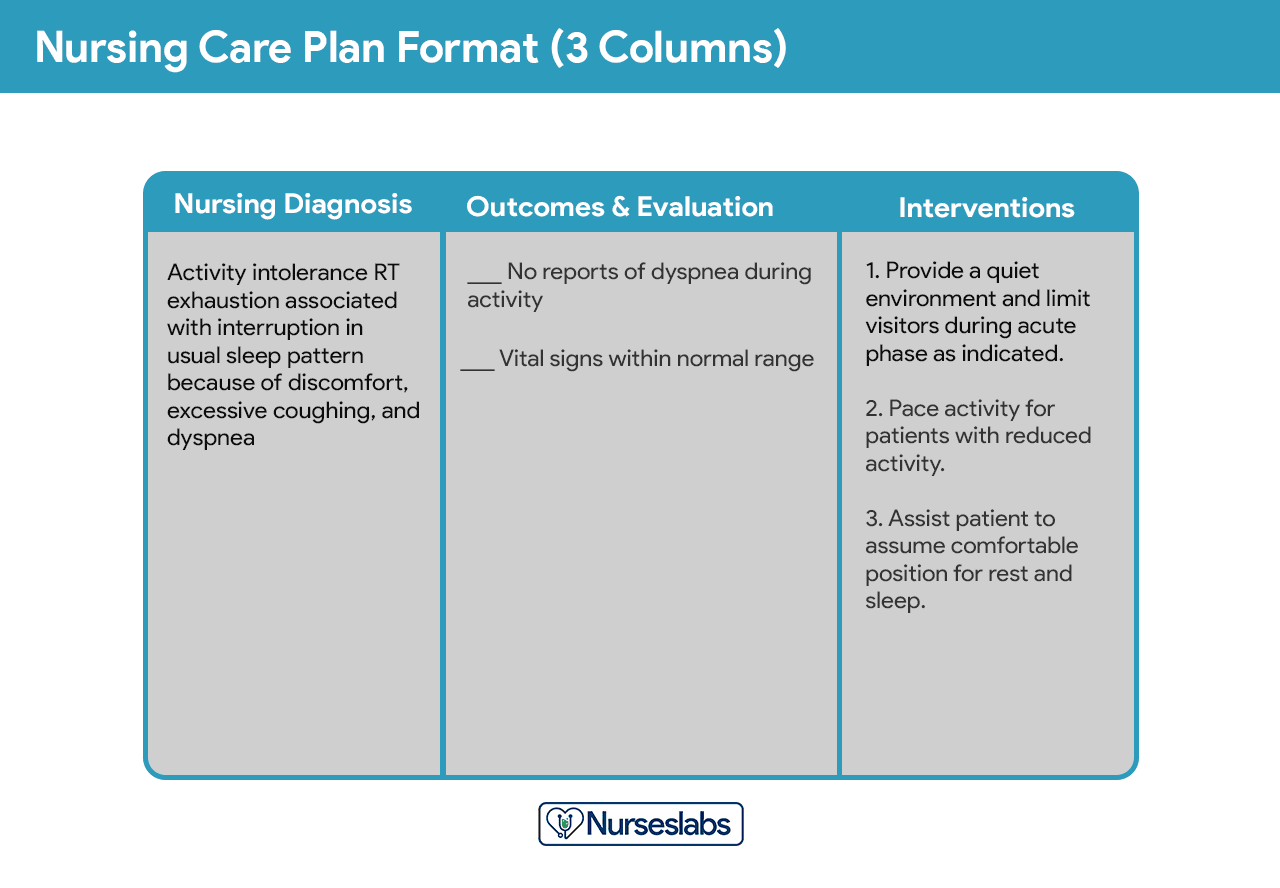
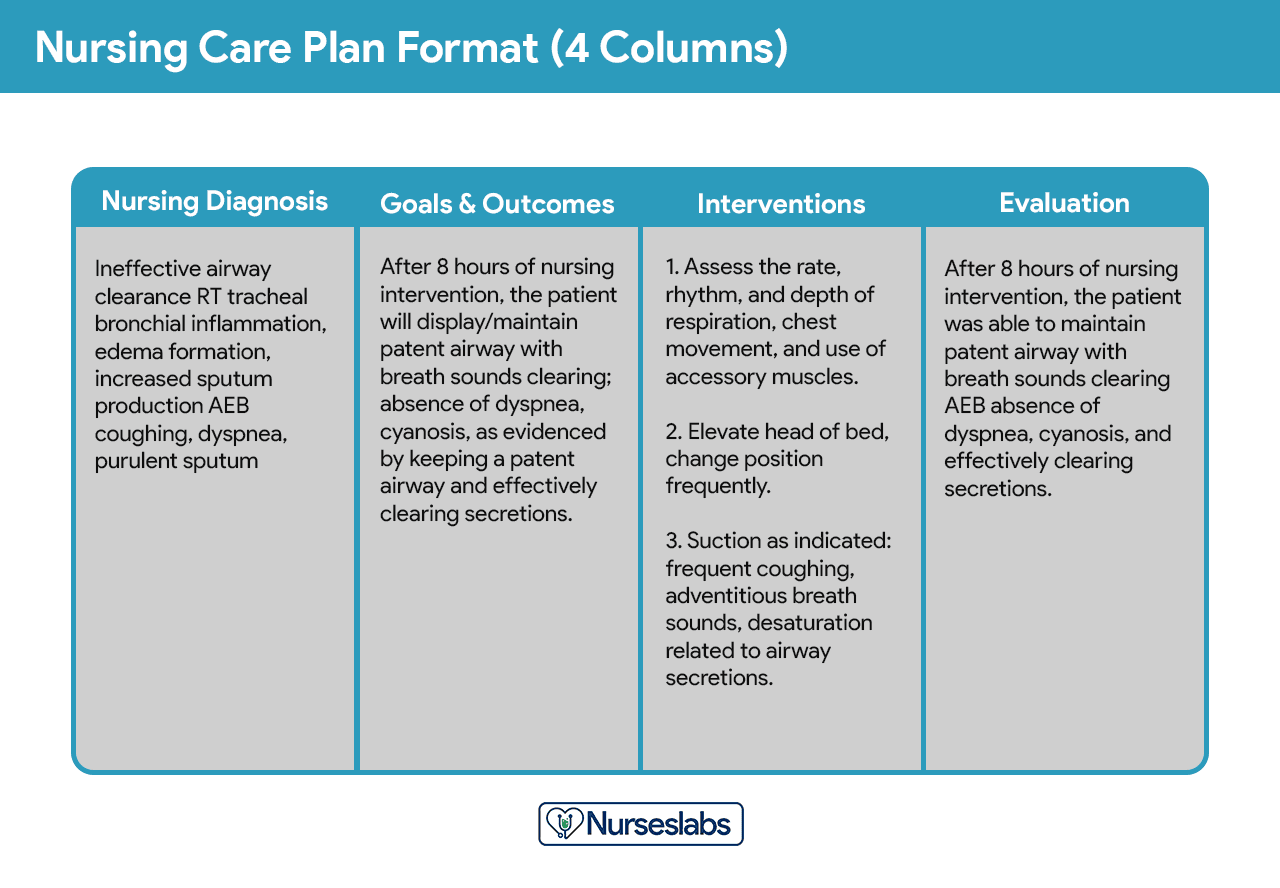
Nursing care plan formats are usually categorized or organized into four columns: (1) nursing diagnoses, (2) desired outcomes and goals, (3) nursing interventions, and (4) evaluation. Some agencies use a three-column plan wherein goals and evaluation are in the same column. Other agencies have a five-column plan that includes a column for assessment cues.
Below is a document containing sample templates for the different nursing care plan formats. Please feel free to edit, modify, and share the template.
Download: Printable Nursing Care Plan Templates and Formats
Student Care Plans
Student care plans are more lengthy and detailed than care plans used by working nurses because they are a learning activity for the students.

Care plans by student nurses are usually required to be handwritten and have an additional column for "Rationale" or "Scientific Explanation" after the nursing interventions column. Rationales are scientific principles that explain the reasons for selecting a particular nursing intervention.
Writing a Nursing Care Plan
How do you write a nursing care plan (NCP)? Just follow the steps below to develop a care plan for your client.
Step 1: Data Collection or Assessment
The first step in writing a nursing care plan is to create a client database using assessment techniques and data collection methods (physical assessment, health history, interview, medical records review, diagnostic studies). A client database includes all the health information gathered. In this step, the nurse can identify the related or risk factors and defining characteristics that can be used to formulate a nursing diagnosis. Some agencies or nursing schools have specific assessment formats you can use.
Step 2: Data Analysis and Organization
Now that you have information about the client's health analyze, cluster, and organize the data to formulate your nursing diagnosis, priorities, and desired outcomes.
Step 3: Formulating Your Nursing Diagnoses
NANDA nursing diagnoses are a uniform way of identifying, focusing on, and dealing with specific client needs and responses to actual and high-risk problems. Actual or potential health problems that can be prevented or resolved by independent nursing intervention are termed nursing diagnoses. We've detailed the steps on how to formulate your nursing diagnoses in this guide:Nursing Diagnosis (NDx): Complete Guide and List
Step 4: Setting Priorities
Setting priorities deals with establishing a preferential sequence for addressing nursing diagnoses and interventions. In this step, the nurse and the client begin planning which nursing diagnosis requires attention first. Diagnoses can be ranked and grouped as having a high, medium, or low priority. Life-threatening problems should be given high priority.
A nursing diagnosis encompasses Maslow's Hierarchy of Needs and helps to prioritize and plan care based on patient-centered outcomes. In 1943, Abraham Maslow developed a hierarchy based on basic fundamental needs innate to all individuals. Basic physiological needs/goals must be met before higher needs/goals can be achieved, such as self-esteem and self-actualization. Physiological and safety needs provide the basis for implementing nursing care and nursing interventions. Thus, they are at the base of Maslow's pyramid, laying the foundation for physical and emotional health.
Maslow's Hierarchy of Needs
- Basic Physiological Needs: Nutrition (water and food), elimination (Toileting), airway (suction)-breathing (oxygen)-circulation (pulse, cardiac monitor, blood pressure) (ABCs), sleep, sex, shelter, and exercise.
- Safety and Security: Injury prevention (side rails, call lights, hand hygiene, isolation, suicide precautions, fall precautions, car seats, helmets, seat belts), fostering a climate of trust and safety (therapeutic relationship), patient education (modifiable risk factors for stroke, heart disease).
- Love and Belonging: Foster supportive relationships, methods to avoid social isolation (bullying), employ active listening techniques, therapeutic communication, and sexual intimacy.
- Self-Esteem: Acceptance in the community, workforce, personal achievement, sense of control or empowerment, accepting one's physical appearance or body habitus.
- Self-Actualization: Empowering environment, spiritual growth, ability to recognize the point of view of others, reaching one's maximum potential.
The client's health values and beliefs, priorities, resources available, and urgency are factors the nurse must consider when assigning priorities. Involve the client in the process to enhance cooperation.
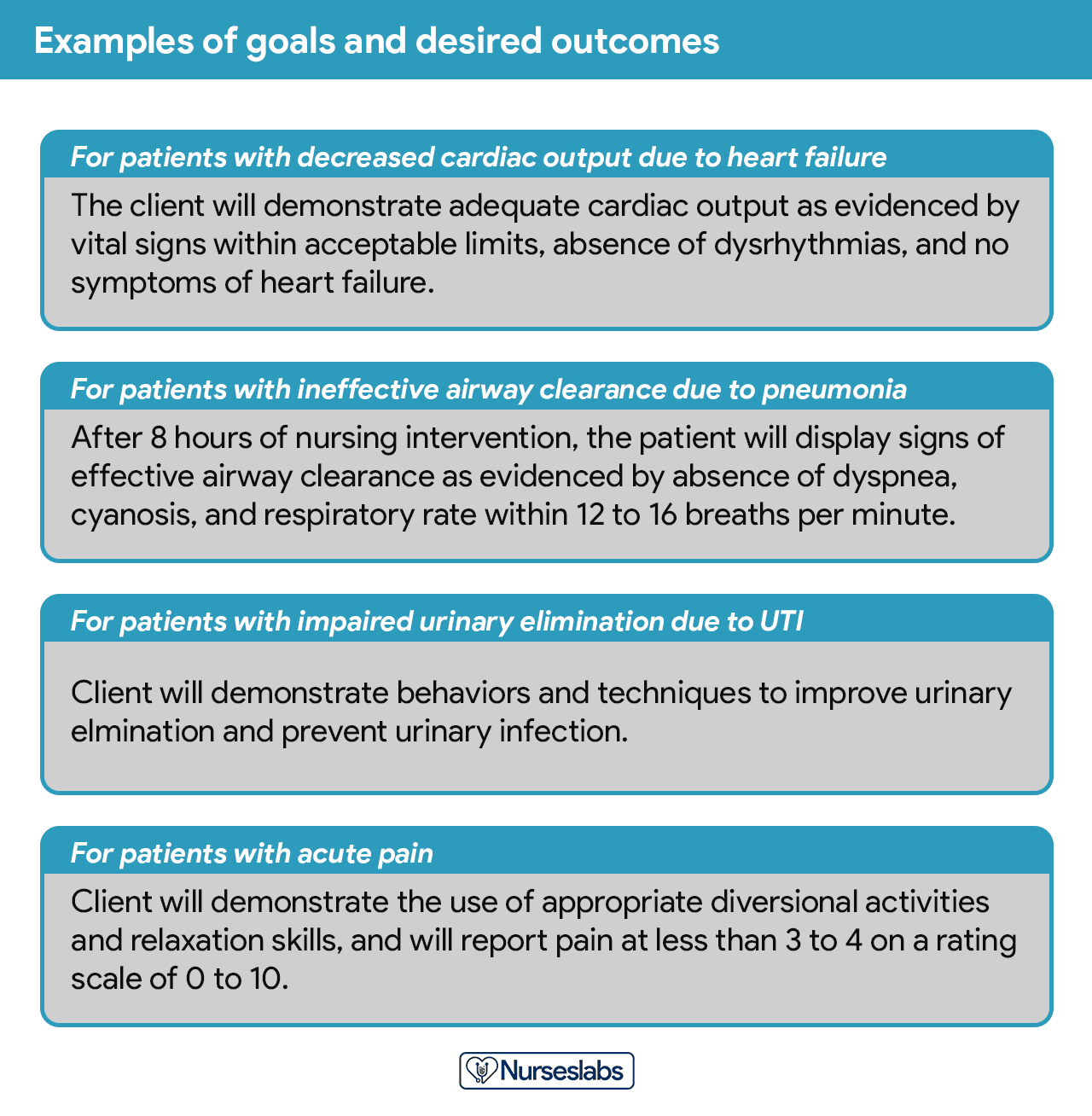
Step 5: Establishing Client Goals and Desired Outcomes
After assigning priorities for your nursing diagnosis, the nurse and the client set goals for each determined priority. Goals or desired outcomes describe what the nurse hopes to achieve by implementing the nursing interventions derived from the client's nursing diagnoses. Goals provide direction for planning interventions, serve as criteria for evaluating client progress, enable the client and nurse to determine which problems have been resolved, and help motivate the client and nurse by providing a sense of achievement.
One overall goal is determined for each nursing diagnosis. The terms goal, outcome, and expected outcome are often used interchangeably.
According to Hamilton and Price (2013), goals should be SMART. SMART goals analysis strategy stands for – Specific, Measurable, Attainable, Realistic, and Time-Bound goals.
- Specific. It should be clear, significant, and sensible for a goal to be effective.
- Measurable or Meaningful. Making sure a goal is measurable makes it easier to monitor progress and know when it reaches the desired result.
- Attainable or Action-Oriented. Goals should be flexible but remain possible.
- Realistic or Results-Oriented. This is important to look forward to effective and successful outcomes by keeping in mind the available resources at hand.
- Timely or Time-Oriented. Every goal needs a designated time parameter, a deadline to focus on, and something to work toward.
Hogston (2011) suggests using the REEPIG standards to ensure that care is of the highest standards. By this means, nursing care plans should be:
- Realistic. Given available resources.
- Explicitly stated. Be clear in precisely what must be done so there is no room for misinterpretation of instructions.
- Evidence-based. That there is research that supports what is being proposed.
- Prioritized. The most urgent problems being dealt with first.
- Involve. Involve both the patient and other members of the multidisciplinary team who are going to be involved in implementing the care.
- Goal centered. That the care planned will meet and achieve the goal set.
Short Term and Long Term Goals
Goals and expected outcomes must be measurable and client-centered. Goals are constructed by focusing on problem prevention, resolution, and rehabilitation. Goals can be short-term or long-term. Most goals are short-term in an acute care setting since much of the nurse's time is spent on the client's immediate needs. Long-term goals are often used for clients who have chronic health problems or live at home, nursing homes, or in extended-care facilities.
- Short-term goal. A statement distinguishing a shift in behavior that can be completed immediately, usually within a few hours or days.
- Long-term goal. Indicates an objective to be completed over a longer period, usually over weeks or months.
- Discharge planning. Involves naming long-term goals, therefore promoting continued restorative care and problem resolution through home health, physical therapy, or various other referral sources.
Components of Goals and Desired Outcomes
Goals or desired outcome statements usually have four components: a subject, a verb, conditions or modifiers, and a criterion of desired performance.
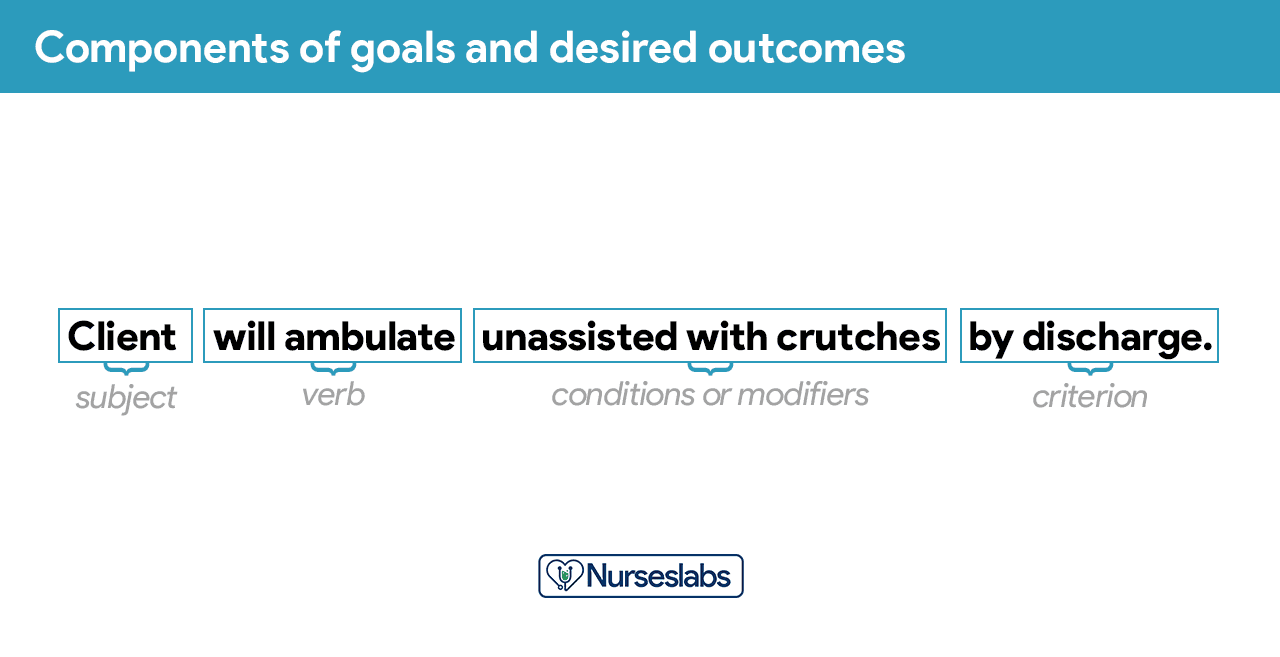
- Subject. The subject is the client, any part of the client, or some attribute of the client (i.e., pulse, temperature, urinary output). That subject is often omitted in writing goals because it is assumed that the subject is the client unless indicated otherwise (family, significant other).
- Verb. The verb specifies an action the client is to perform, for example, what the client is to do, learn, or experience.
- Conditions or modifiers. These are the "what, when, where, or how" that are added to the verb to explain the circumstances under which the behavior is to be performed.
- Criterion of desired performance. The criterion indicates the standard by which a performance is evaluated or the level at which the client will perform the specified behavior. These are optional.
When writing goals and desired outcomes, the nurse should follow these tips:
- Write goals and outcomes in terms of client responses and not as activities of the nurse. Begin each goal with "Client will […]" help focus the goal on client behavior and responses.
- Avoid writing goals on what the nurse hopes to accomplish, and focus on what the client will do.
- Use observable, measurable terms for outcomes. Avoid using vague words that require interpretation or judgment of the observer.
- Desired outcomes should be realistic for the client's resources, capabilities, limitations, and on the designated time span of care.
- Ensure that goals are compatible with the therapies of other professionals.
- Ensure that each goal is derived from only one nursing diagnosis. Keeping it this way facilitates evaluation of care by ensuring that planned nursing interventions are clearly related to the diagnosis set.
- Lastly, make sure that the client considers the goals important and values them to ensure cooperation.
Step 6: Selecting Nursing Interventions
Nursing interventions are activities or actions that a nurse performs to achieve client goals. Interventions chosen should focus on eliminating or reducing the etiology of the nursing diagnosis. As for risk nursing diagnoses, interventions should focus on reducing the client's risk factors. In this step, nursing interventions are identified and written during the planning step of the nursing process; however, they are actually performed during the implementation step.
Types of Nursing Interventions
Nursing interventions can be independent, dependent, or collaborative:
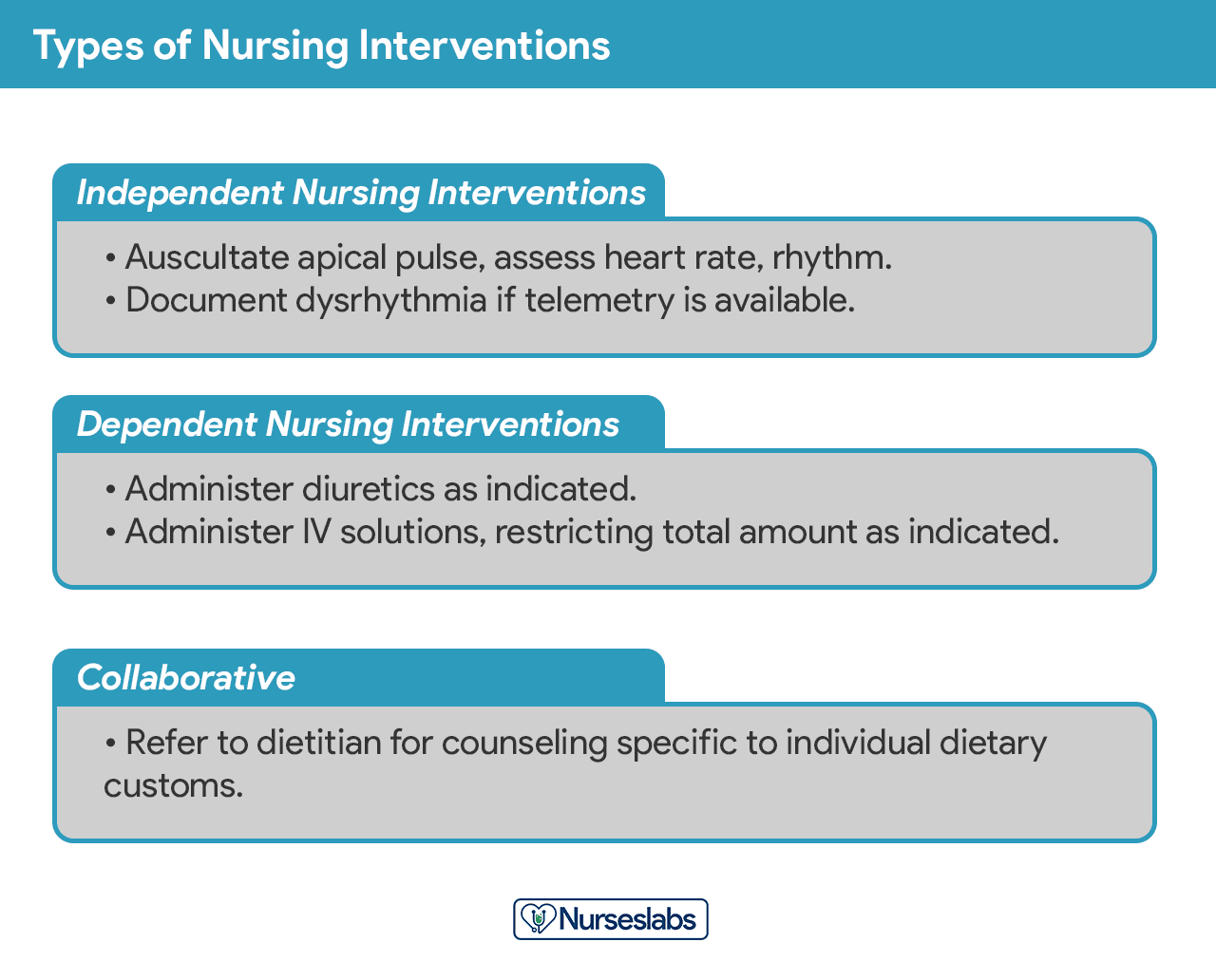
- Independent nursing interventions are activities that nurses are licensed to initiate based on their sound judgement and skills. Includes: ongoing assessment, emotional support, providing comfort, teaching, physical care, and making referrals to other health care professionals.
- Dependent nursing interventions are activities carried out under the physician's orders or supervision. Includes orders to direct the nurse to provide medications, intravenous therapy, diagnostic tests, treatments, diet, and activity or rest. Assessment and providing explanation while administering medical orders are also part of the dependent nursing interventions.
- Collaborative interventions are actions that the nurse carries out in collaboration with other health team members, such as physicians, social workers, dietitians, and therapists. These actions are developed in consultation with other health care professionals to gain their professional viewpoint.
Nursing interventions should be:
- Safe and appropriate for the client's age, health, and condition.
- Achievable with the resources and time available.
- Inline with the client's values, culture, and beliefs.
- Inline with other therapies.
- Based on nursing knowledge and experience or knowledge from relevant sciences.
When writing nursing interventions, follow these tips:
- Write the date and sign the plan. The date the plan is written is essential for evaluation, review, and future planning. The nurse's signature demonstrates accountability.
- Nursing interventions should be specific and clearly stated, beginning with an action verb indicating what the nurse is expected to do. Action verb starts the intervention and must be precise. Qualifiers of how, when, where, time, frequency, and amount provide the content of the planned activity. For example: "Educate parents on how to take temperature and notify of any changes," or "Assess urine for color, amount, odor, and turbidity."
- Use only abbreviations accepted by the institution.
Step 7: Providing Rationale
Rationales, also known as scientific explanations, explain why the nursing intervention was chosen for the NCP.
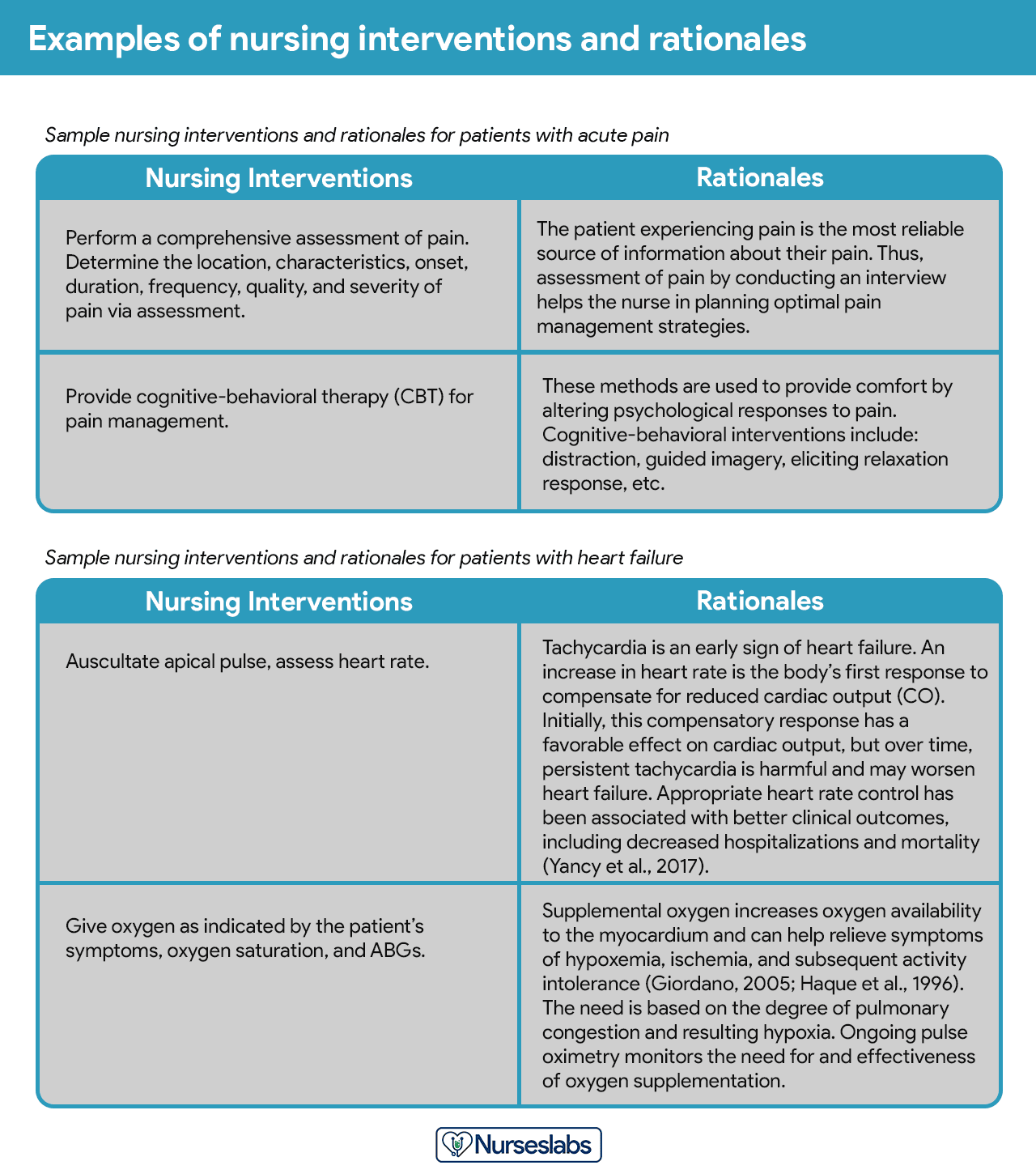
Rationales do not appear in regular care plans. They are included to assist nursing students in associating the pathophysiological and psychological principles with the selected nursing intervention.
Step 8: Evaluation
Evaluating is a planned, ongoing, purposeful activity in which the client's progress towards achieving goals or desired outcomes and the effectiveness of the nursing care plan (NCP). Evaluation is an essential aspect of the nursing process because conclusions drawn from this step determine whether the nursing intervention should be terminated, continued, or changed.
Step 9: Putting it on Paper
The client's care plan is documented according to hospital policy and becomes part of the client's permanent medical record which may be reviewed by the oncoming nurse. Different nursing programs have different care plan formats. Most are designed so that the student systematically proceeds through the interrelated steps of the nursing process, and many use a five-column format.
Nursing Care Plan List
This section lists the sample nursing care plans (NCP) and NANDA nursing diagnoses for various disease and health conditions. They are segmented into categories:
Basic Nursing and General Care Plans
Miscellaneous nursing care plans examples that don't fit other categories:
- Cancer (Oncology Nursing)
- End-of-Life Care (Hospice Care or Palliative)
- Geriatric Nursing (Older Adult)
- Prolonged Bed Rest
- Surgery (Perioperative Client)
- Systemic Lupus Erythematosus
- Total Parenteral Nutrition
Surgery and Perioperative Care Plans
Care plans that involve surgical intervention.
- Amputation
- Appendectomy
- Cholecystectomy
- Fracture UPDATED!
- Hemorrhoids
- Hysterectomy
- Ileostomy & Colostomy
- Laminectomy (Disc Surgery)
- Mastectomy
- Subtotal Gastrectomy
- Surgery (Perioperative Client)
- Thyroidectomy
- Total Joint (Knee, Hip) Replacement
Cardiac Care Plans
Nursing care plans about the different diseases of the cardiovascular system:
- Angina Pectoris (Coronary Artery Disease)
- Cardiac Arrhythmia (Digitalis Toxicity)
- Cardiac Catheterization
- Cardiogenic Shock
- Congenital Heart Disease
- Heart Failure UPDATED!
- Hypertension UPDATED!
- Hypovolemic Shock
- Myocardial Infarction
- Pacemaker Therapy
Endocrine and Metabolic Care Plans
Nursing care plans (NCP) related to the endocrine system and metabolism:
- Acid-Base Balance
- – Respiratory Acidosis
- – Respiratory Alkalosis
- – Metabolic Acidosis
- – Metabolic Alkalosis
- Addison's Disease
- Cushing's Disease
- Diabetes Mellitus Type 1
- Diabetes Mellitus Type 2 UPDATED!
- Diabetic Ketoacidosis (DKA) and Hyperglycemic Hyperosmolar Nonketotic Syndrome (HHNS)
- Eating Disorders: Anorexia & Bulimia Nervosa
- Fluid and Electrolyte Imbalances:
- – Fluid Balance: Hypervolemia & Hypovolemia
- – Potassium (K) Imbalances: Hyperkalemia and Hypokalemia
- – Sodium (Na) Imbalances: Hypernatremia and Hyponatremia
- – Magnesium (Mg) Imbalances: Hypermagnesemia and Hypomagnesemia
- – Calcium (Ca) Imbalances: Hypercalcemia and Hypocalcemia
- Gestational Diabetes Mellitus
- Hyperthyroidism
- Hypothyroidism
- Obesity
- Thyroidectomy
Gastrointestinal
Care plans (NCP) covering the disorders of the gastrointestinal and digestive system:
- Appendectomy
- Cholecystectomy
- Cholecystitis and Cholelithiasis
- Gastroenteritis
- Gastroesophageal Reflux Disease (GERD)
- Hemorrhoids
- Hepatitis
- Ileostomy & Colostomy
- Inflammatory Bowel Disease
- Intussusception
- Liver Cirrhosis
- Pancreatitis
- Peritonitis
- Peptic Ulcer Disease
- Subtotal Gastrectomy
Genitourinary
Care plans related to the reproductive and urinary system disorders:
- Acute Glomerulonephritis
- Acute Renal Failure
- Benign Prostatic Hyperplasia (BPH)
- Chronic Renal Failure
- Hemodialysis
- Hysterectomy
- Mastectomy
- Menopause
- Nephrotic Syndrome
- Peritoneal Dialysis
- Prostatectomy
- Urolithiasis (Renal Calculi)
- Urinary Tract Infection
- Vesicoureteral Reflux (VUR)
Hematologic and Lymphatic
Care plans related to the hematologic and lymphatic system:
- Anaphylactic Shock
- Anemia UPDATED!
- Aortic Aneurysm
- Deep Vein Thrombosis
- Disseminated Intravascular Coagulation
- Hemophilia
- Leukemia
- Lymphoma
- Sepsis and Septicemia
- Sickle Cell Anemia Crisis
Infectious Diseases
NCPs for communicable and infectious diseases:
- Acquired Immunodeficiency Syndrome (AIDS) (HIV Positive)
- Acute Rheumatic Fever
- Dengue Hemorrhagic Fever
- Herpes Zoster (Shingles)
- Influenza (Flu)
- Pulmonary Tuberculosis
Integumentary
All about disorders and conditions affecting the integumentary system:
- Burn Injury
- Dermatitis
- Herpes Zoster (Shingles)
- Pressure Ulcer (Bedsores)
Maternal and Newborn Care Plans
Nursing care plans about the care of the pregnant mother and her infant. See care plans for maternity and obstetric nursing:
- Abruptio Placenta
- Cesarean Birth UPDATED!
- Cleft Palate and Cleft Lip
- Dysfunctional Labor (Dystocia)
- Elective Termination
- Gestational Diabetes Mellitus UPDATED!
- Hyperbilirubinemia
- Labor Stages, Induced and Augmented Labor
- Neonatal Sepsis
- Perinatal Loss
- Placenta Previa
- Postpartum Hemorrhage UPDATED!
- Postpartum Thrombophlebitis
- Prenatal Hemorrhage
- Precipitous Labor
- Preeclampsia and Gestational Hypertensive Disorders UPDATED!
- Premature Dilation of the Cervix
- Prenatal Infection
- Preterm Labor
- Puerperal Infection
- Substance Abuse in Pregnancy
Mental Health and Psychiatric
Care plans for mental health and psychiatric nursing:
- Alcohol Withdrawal
- Anxiety and Panic Disorders
- Bipolar Disorders
- Major Depression
- Personality Disorders
- Schizophrenia
- Sexual Assault
- Substance Dependence and Abuse
- Suicide Behaviors
Musculoskeletal
Care plans related to the musculoskeletal system:
- Amputation
- Congenital Hip Dysplasia
- Fracture UPDATED!
- Juvenile Rheumatoid Arthritis
- Laminectomy (Disc Surgery)
- Osteoarthritis
- Osteoporosis
- Rheumatoid Arthritis
- Scoliosis
- Spinal Cord Injury
- Total Joint (Knee, Hip) Replacement
Neurological
Nursing care plans (NCP) for related to nervous system disorders:
- Alzheimer's Disease UPDATED!
- Brain Tumor
- Cerebral Palsy
- Cerebrovascular Accident (Stroke) UPDATED!
- Guillain-Barre Syndrome
- Meningitis
- Multiple Sclerosis
- Parkinson's Disease
- Seizure Disorder
- Spinal Cord Injury
Ophthalmic
Care plans relating to eye disorders:
- Cataracts
- Glaucoma
- Macular Degeneration
Pediatric Nursing Care Plans
Nursing care plans (NCP) for pediatric conditions and diseases:
- Acute Glomerulonephritis
- Acute Rheumatic Fever
- Apnea
- Benign Febrile Convulsions
- Brain Tumor
- Bronchiolitis
- Bronchopulmonary Dysplasia (BPD)
- Cardiac Catheterization
- Cerebral Palsy
- Child Abuse
- Cleft Lip and Cleft Palate
- Congenital Heart Disease
- Congenital Hip Dysplasia
- Croup Syndrome
- Cryptorchidism (Undescended Testes)
- Cystic Fibrosis
- Diabetes Mellitus Type 1
- Dying Child
- Epiglottitis
- Febrile Seizure
- Guillain-Barre Syndrome
- Hospitalized Child
- Hydrocephalus
- Hypospadias and Epispadias
- Intussusception
- Juvenile Rheumatoid Arthritis
- Kawasaki Disease
- Meningitis
- Nephrotic Syndrome
- Osteogenic Sarcoma (Osteosarcoma)
- Otitis Media
- Scoliosis
- Spina Bifida
- Tonsillitis and Adenoiditis
- Umbilical and Inguinal Hernia
- Vesicoureteral Reflux (VUR)
- Wilms Tumor (Nephroblastoma)
Respiratory
Care plans for respiratory system disorders:
- Asthma
- Bronchiolitis
- Bronchopulmonary Dysplasia (BPD)
- Chronic Obstructive Pulmonary Disease (COPD)
- Cystic Fibrosis
- Hemothorax and Pneumothorax
- Influenza (Flu)
- Lung Cancer
- Mechanical Ventilation
- Near-Drowning
- Pleural Effusion
- Pneumonia
- Pulmonary Embolism
- Pulmonary Tuberculosis
- Tracheostomy
References and Sources
Recommended reading materials and sources for this NCP guide:
- Ackley, B. J., Ladwig, G. B., Makic, M. B., Martinez-Kratz, M., & Zanotti, M. (2019).Nursing diagnosis handbook e-book: an evidence-based guide to planning care. Elsevier Health Sciences.
- Björvell, C., Thorell-Ekstrand, I., & Wredling, R. (2000). Development of an audit instrument for nursing care plans in the patient record.BMJ Quality & Safety,9(1), 6-13. [Link]
- Carpenito-Moyet, L. J. (2009).Nursing care plans & documentation: nursing diagnoses and collaborative problems. Lippincott Williams & Wilkins.
- DeLaune, S. C., & Ladner, P. K. (2011).Fundamentals of nursing: Standards and practice. Cengage learning.
- Gulanick, M., & Myers, J. L. (2016). Nursing Care Plans: Diagnoses, Interventions, and Outcomes . Elsevier Health Sciences. [Link]
- Lee, T. T. (2004). Evaluation of computerized nursing care plan: instrument development.Journal of Professional Nursing,20(4), 230-238.
- Lee, T. T. (2006). Nurses' perceptions of their documentation experiences in a computerized nursing care planning system.Journal of Clinical Nursing,15(11), 1376-1382.
- Rn, B. O. C., Rn, H. M., Rn, D. T., & Rn, F. E. (2000). Documenting and communicating patient care: Are nursing care plans redundant?.International Journal of Nursing Practice,6(5), 276-280.
- Stonehouse, D. (2017). Understanding the nursing process.British Journal of Healthcare Assistants,11(8), 388-391.
- Yildirim, B., & Ozkahraman, S. (2011). Critical thinking in nursing process and education.International journal of humanities and social science,1(13), 257-262.
Source: https://nurseslabs.com/nursing-care-plans/
0 Response to "Beat Easy to Cheat on Care Plan"
Post a Comment